Monitoring AFib (AF)
What is AF? Why should I monitor for afib?
AF stands for Atrial Fibrillation, or afib. AF is an abnormal heart rhythm sometimes referred as an irregular heart beat. Normally our hearts beat regularly. An average heart beats about 70 times per minute (beats per minute, or bpm), or a little more than once per second. Those 70 heart beats each minute are all evenly spaced out and they are predictable, like the drumbeat of a song. If you have a normal heart rhythm and you feel your own pulse, you will see that your pulse taps out a regular, predictable beat. Each time your heart beats, it squeezes a small amount of blood forward into your arteries.  This squeeze causes the arteries to stretch out a little with each heart beat. This brief stretching of the arteries is called an arterial pulsation. When you feel your pulse, what you are feeling is the artery pulsating – expanding or stretching – a little bit with each heart beat, due to the blood which the heart squeezed into it during that heart beat. The arterial pulsation keeps time exactly with the heart beat itself. Each time the heart beats, all the arteries in the body pulsate. That is why the pulse rate is the same as the heart rate. We can say that the average heart rate is 70 bpm, or that the average pulse rate is 70 bpm – it means the same thing because each single heart beat causes a single arterial pulsation
This squeeze causes the arteries to stretch out a little with each heart beat. This brief stretching of the arteries is called an arterial pulsation. When you feel your pulse, what you are feeling is the artery pulsating – expanding or stretching – a little bit with each heart beat, due to the blood which the heart squeezed into it during that heart beat. The arterial pulsation keeps time exactly with the heart beat itself. Each time the heart beats, all the arteries in the body pulsate. That is why the pulse rate is the same as the heart rate. We can say that the average heart rate is 70 bpm, or that the average pulse rate is 70 bpm – it means the same thing because each single heart beat causes a single arterial pulsation
Our natural pacemaker
The heart’s beating is controlled electrically. Everybody has a natural pacemaker in their heart that tells the heart when to beat. This natural pacemaker is called the sinus node. The sinus node sends out an electrical signal at regular intervals which tells the heart to beat. We can see this electrical signal on an electrocardiogram. An electrocardiogram, sometimes abbreviated ECG (or EKG, referring to the German spelling of the word cardio – kardio) simply measures the electrical signals of the heart, not the actual heart beat or pulse. Because each electrical signal to beat causes one heart beat, and each heart beat causes one arterial pulsation, we usually consider all three to be equal. In other words, the ECG electrical heart rate = the heart beat = the arterial pulse. Because the pulse rate or heart rate is controlled by the heart’s electrical system, any problems with the electrical system will cause problems with the pulse or heart rate. For example, if the electrical system generates signals too fast, then the heart will beat too fast. If it sends out electrical signals too slowly, then the heart will beat too slowly. Or, in the case of atrial fibrillation (AF or AFib) when the electrical system sends out signals irregularly, then the heart will beat irregularly.
What does it mean for the heart to beat irregularly?
During a normal heart beat, there is a synchronized electrical signal which tells the heart muscle to contract in unison, causing a single heart beat. Think of it like a long crew row boat. The electrical signal is like the coxswain who gives the order to row. The individual rowers are like the heart muscle. Following the coxswain’s command each rower rows a stroke, all in unison, and their collective action pulls the boat forward. If the  coxswain were to stop doing their job, and each rower were to row randomly on their own, all at different times and in different directions, then the boat wouldn’t go anywhere. A similar thing can happen in the heart if the electrical system goes offline and instead of generating a synchronized signal, simply generates jumbled, random electrical noise. Let’s look at what happens in the heart’s atriums, the two upper chambers of the heart, which are the first to squeeze during each heart beat. Normally, each muscle cell in the atriums squeezes simultaneously, like all the rowers rowing together in the crew boat. But when the electrical signal degenerates into only incoherent noise, then each muscle cell contracts randomly, at different times and different strengths. This results in the atria quivering continuously instead of a unified contraction. We call that quivering “fibrillating.” The atria are not contracting, they are just fibrillating. We call that atrial fibrillation.
coxswain were to stop doing their job, and each rower were to row randomly on their own, all at different times and in different directions, then the boat wouldn’t go anywhere. A similar thing can happen in the heart if the electrical system goes offline and instead of generating a synchronized signal, simply generates jumbled, random electrical noise. Let’s look at what happens in the heart’s atriums, the two upper chambers of the heart, which are the first to squeeze during each heart beat. Normally, each muscle cell in the atriums squeezes simultaneously, like all the rowers rowing together in the crew boat. But when the electrical signal degenerates into only incoherent noise, then each muscle cell contracts randomly, at different times and different strengths. This results in the atria quivering continuously instead of a unified contraction. We call that quivering “fibrillating.” The atria are not contracting, they are just fibrillating. We call that atrial fibrillation.
The heart’s atria, or upper chambers, are not responsible for the heart’s squeezing of blood out to the rest of the body – they do not cause the arterial pulsation. That is caused by the much larger and stronger lower chambers of the heart called the ventricles. The ventricles wait to beat until after the atria beat. The electrical signal passes through the atria, causing them to beat, and then continues to the ventricles, causing them to beat. During atrial fibrillation, the atria are simply fibrillating, not contracting. Our hearts have a failsafe mechanism which protects the ventricles from fibrillating during this situation. There is an electrical filter between the atria and the ventricles which prevents the disorganized electrical noise from propagating through to the ventricles and causing them to fibrillate as well. This filter is called the atrioventricular node, or AV node. The AV node blocks all the fibrillatory electrical signals and lets only a single unified signal through, so that the ventricles still contract together in a unified heart beat. But when the atriums are fibrillating, the electrical signal goes through the AV node to the ventricles at completely random intervals. This causes the ventricles to contract at random intervals. And that causes the arterial pulse to also become random. That is why if you feel the pulse of someone who has atrial fibrillation, you will feel the pulse to beat fast for a few beats, then slow, then fast, etc. And that is why AF is sometimes called an “irregular heart beat.” The heart’s squeezing of the blood is just as strong as it was before, because the ventricles are still squeezing the blood out normally with each beat. But the ventricular beats (and therefore the arterial pulsations) come at random intervals because of the electrical fibrillation in the atria.
So what if the heart beats irregularly?
There are two main issues with AF. The first is that when the heart beats randomly, it can end up beating too fast (afib with RVR, rapid ventricular response) or too slow. Normally, the heart’s synchronized electrical signal speeds up or slows down according to the body’s needs. For example, when you are resting your pulse will be slower, and when you are running it will be faster. However, during atrial fibrillation, the electrical signals are all jumbled and can no longer adequately control the heart rate. Therefore, the heart can end up beating too slow or too fast. This can cause symptoms of palpitations or a feeling of the heart racing even when you are just resting, if the heart is beating too fast (afib with RVR.) Or it can cause dizziness or even fainting if the heart is beating too slowly.
The second issue with AF concerns the blood flow in the atria. Normally, when the electrical signal is synchronized appropriately, the atria contract in unison, squeezing the blood into the ventricles. Then the ventricles contract, squeezing the blood out to the arteries which carry the blood to the rest of the body. In AF, because the atria are not actually contracting, but are only fibrillating, or quivering, the blood does not get squeezed or pumped though quickly like it should. The blood can swirl around inside the atria for a while before randomly finding its way down into the ventricles, where it will then be squeezed or pumped out to the rest of the body. Whenever blood stays too long in one place, there is a risk of that blood forming a blood clot. In atrial fibrillation there is a risk of forming blood clots inside the atria because the blood stays inside the atria longer than it should. And if a blood clot forms inside the atria, a piece of that blood clot can break off and flow through to the ventricles where it can get pumped out into the arteries. It will then eventually become lodged inside an artery somewhere in the body, blocking that artery and blocking blood flow to that part of the body. If that happens in an artery in the brain, it can cause a stroke.
I don’t want to faint or have palpitations or have a stroke. How can I prevent that?
The first step is simply to find out if you have AF. If you don’t, then you don’t have to worry about it. That’s not to say that it’s impossible to have palpitations or fainting or a stroke from something other than AFib. But if you don’t have AF then your chances of having any of those things is much lower. The main way to check if someone has AF is to check either their ECG, which measures the electrical activity of the heart and can see if the electrical activity is normal or fibrillatory, or to check the pulse and see if its irregular. If and ECG shows normal synchronized electrical activity or if the pulse is regular, then you don’t have AF. The trouble with AF is that it can come and go. In other words, the electrical system of the heart can be normal sometimes and disorganized/fibrillatory at other times. We call this paroxysmal atrial fibrillation. A paroxysm is just a fancy word that means an episode. Paroxysmal AF is just the medical term for episodic AF. The trouble with that is that just because your pulse is regular at the time you check it, it might not be regular at other times when you’re not checking it. And even with paroxysmal AF, or PAF, there is still a chance of having a blood clot in the atrium and therefore a stroke. This means that when someone is suspected of having AF or PAF, they must be monitored for a very long time. Usually people are monitored for either an entire day, sometimes an entire week or two. Sometimes people need to be monitored even longer, up to even a few years.
How do we monitor for afib?
Holter monitors
Most traditional monitors for AF are electrical monitors. A typical electrical monitor uses several wires, called leads, attached to the chest wall with small stickers. All of the wires are connected to a small box which records and stores the electrical signals. 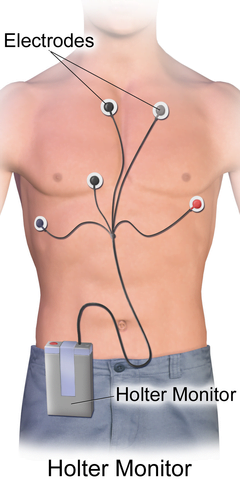 The box with the wires is worn typically for a day or two, up to a couple of weeks, and then returned to the doctor where the stored electrical signals are read to see if there are any irregular signals which look like AF. The recorded signals in modern monitors like this are usually time-stamped so that if you are wearing a monitor and have a particular symptoms at, say, 11AM, you can record that symptom in a diary. That way, when you turn in the afib monitor to the doctor he or she can look through the recordings and can see exactly what your heart was doing electrically at 11AM, to see if your symptom was related to an abnormal heart rhythm. Monitors like this are called holter monitors and are in use today. They are somewhat bulky due to the box and the wires, and difficult to sleep with, cannot be worn in water or rain, and are difficult to wear during sporting activities or when sweating because the stickers can come off if the person sweats a lot. Holter monitors also do not give real-time information, but rather simply collect the data which is read by the doctor later.
The box with the wires is worn typically for a day or two, up to a couple of weeks, and then returned to the doctor where the stored electrical signals are read to see if there are any irregular signals which look like AF. The recorded signals in modern monitors like this are usually time-stamped so that if you are wearing a monitor and have a particular symptoms at, say, 11AM, you can record that symptom in a diary. That way, when you turn in the afib monitor to the doctor he or she can look through the recordings and can see exactly what your heart was doing electrically at 11AM, to see if your symptom was related to an abnormal heart rhythm. Monitors like this are called holter monitors and are in use today. They are somewhat bulky due to the box and the wires, and difficult to sleep with, cannot be worn in water or rain, and are difficult to wear during sporting activities or when sweating because the stickers can come off if the person sweats a lot. Holter monitors also do not give real-time information, but rather simply collect the data which is read by the doctor later.
MCT monitors
A more advanced type of cardiac event monitor is called an MCT monitor, or mobile cardiac telemetry monitor. This is very similar to a holter monitor in that it has the same box, wires, and stickers. The main difference between a regular holter monitor and an MCT is in the technology inside the box. The MCT monitor has an antenna inside the box which is connected usually through a cellular data network so that a monitoring center can see the data in real time as it is collected. This means that an MCT monitor can give real time data and can be configured to send your doctor alerts in real time if an abnormal rhythm is detected. MCTs suffer from the same wearing restrictions that holter monitors do, however, such as avoiding sweaty activities, avoiding water, general bulkiness, and difficulty with sleeping.
Patch type monitors
A newer type of electrical heart rhythm monitor is a patch-type monitor. These monitors are self-contained inside of a much smaller metal box, and they don’t have any wires. These monitors are made of metal so that the actual metal on the outside of the box acts as one of the wire leads in the older holter monitors. This means that a patch monitor gathers its electrical data directly from the walls of the box itself. The entire small metal box is encased in a large patch-type sticker which sticks the metal box to the patient’s chest wall. A holter monitor or an MCT monitor has several wires. These wires are placed in different places on the chest wall, and each one can “see” the electrical data from the heart from a different direction. That means that if the electrical signal happens to look fuzzy or any way difficult to interpret in one of the leads, the physician can look at one of the other leads for confirmation.  This helps with the accuracy of the test. The patch monitors sacrifice this redundancy for convenience. They only receive data from the wall of the box, equivalent to a single lead in a holter monitor or MCT, but they are much more convenient because they don’t have any wires or external boxes hanging around – they are just literally stuck right onto the patient. Patch type monitors are typically worn for up to two weeks and are then returned to the doctor to have the recordings analyzed.
This helps with the accuracy of the test. The patch monitors sacrifice this redundancy for convenience. They only receive data from the wall of the box, equivalent to a single lead in a holter monitor or MCT, but they are much more convenient because they don’t have any wires or external boxes hanging around – they are just literally stuck right onto the patient. Patch type monitors are typically worn for up to two weeks and are then returned to the doctor to have the recordings analyzed.
ILRs
There are even patch type monitors that are so small that they can be surgically implanted just under the skin on the chest wall. That way, they can monitor the heart all the time and the patient doesn’t have anything at all outside their body to worry about. The battery on one of these internal monitors, called implantable or insertable loop recorders, or ILRs, can last for up to three years. ILRs can be removed at any time by another minor surgical procedure. ILRs are invasive and require a surgical procedure and this certainly limits their appeal and usefulness. But they have the benefit of being able to record for the longest amount of time of the current generation of electrical heart rate monitors, and have the benefit of being able to record during all types of activity, including sports, swimming, sleep, etc, since there are no external parts to worry about. ILRs communicate their recordings wirelessly to a small console usually kept in the patient’s bedroom which relays the information to the doctor. Reports are usually generated automatically every month, but can be generated more frequently depending on the patient’s symptoms.
Pulse monitors
Modern technology has allowed a variety of sensors to be constructed in a very small size. This has allowed for accurate monitoring of the pulse as a way to detect abnormal heart rhythms instead of monitoring the electrical signals in the heart itself. This means that the trade-off made by the patch-type monitors and ILRs no longer has to be made. Recall that because the patch monitors and ILRs don’t have any wires they only can see the equivalent of a single electrical lead. If the signal is not good in that lead, they are stuck, and their accuracy is reduced. They made that sacrifice for the sake of convenience. With pulse-type monitors, that sacrifice doesn’t have to be made. Pulse monitors are small devices that measure one’s pulse and therefore don’t rely on electrical signals or leads.
Atrial
One kind of pulse type monitor is the typical pulse oximeter (spo2 monitor or pulse ox monitor) that your doctor uses to measure your blood’s oxygen level. This device is a small clip into which you insert one of your fingers.  Inside the device is a sensor which uses reflected light passing through the skin of your finger to detect the oxygen level in your blood. These sensors can also detect your pulse rate. They have a small display on the top of the clip which usually will display both the oxygen level, for example 98%, as well as your pulse rate, for example 84bpm. Many modern home blood pressure cuffs incorporate a similar feature, where they will display both your blood pressure and also your pulse rate. Some more advanced models will even have a display feature which will alert the user that their pulse rhythm may be irregular.
Inside the device is a sensor which uses reflected light passing through the skin of your finger to detect the oxygen level in your blood. These sensors can also detect your pulse rate. They have a small display on the top of the clip which usually will display both the oxygen level, for example 98%, as well as your pulse rate, for example 84bpm. Many modern home blood pressure cuffs incorporate a similar feature, where they will display both your blood pressure and also your pulse rate. Some more advanced models will even have a display feature which will alert the user that their pulse rhythm may be irregular.
CardiacSense Medical Watch
The CSMW is many monitors built into one (respiratory monitor, sleep apnea monitor, oxygen saturation monitor, home blood pressure monitor, cardiac event monitor, afib monitor and more) and it incorporates an advanced pulse monitor as well. In this way it is able to monitor a patient’s pulse in real time, all the time. By monitoring the pulse consistently, the CSMW is able to detect abnormal heart rhythms. The CSMW may be connected to the patient’s smartphone, allowing the patient to view reports and send reports to the physician. The sensors and algorithms within the CSMW are extremely accurate at detecting AF and have been CE-marked for this purpose and currently going through the FDA approval process. This means that the CSMW is the first pulse monitor which can function as a non-invasive long-term monitor in order to accurately detect AF and even PAF which may occur only rarely but nonetheless may still cause atrial blood clots and therefore strokes. Unlike holter monitors, MCT monitors and patch monitors, which can only monitor for a maximum of approximately one month, the CSMW can monitor forever (with the exception of small breaks to recharge the watch battery). And unlike ILRs, the CSMW is simply worn on the wrist and does not require any surgical procedures.